[
editing in red is mine]
In this update:
[1] UK - HPA investigation findings, Eurosurveillance
[2] UK - Clinical and laboratory findings, Eurosurveillance
[3] Saudi Arabia - ongoing investigations, newswire
[4] USA - current recommendations, MMWR
******
[1] UK - HPA investigation findings, Eurosurveillance
Date: 4 Oct 2012
Source: Eurosurveillance Volume 17, Issue 40, 4 Oct 2012 [edited]
http://eurosurveillance.org/ViewArticle.aspx?ArticleId=20292
Rapid communications
The United Kingdom Public Health response to an imported laboratory confirmed case of a novel coronavirus in September 2012
--------------------------
On
[22 Sep 2012], a novel coronavirus, very closely related to that from a
fatal case in Saudi Arabia 3 months previously, was detected in a
previously well adult transferred to intensive care in London from Qatar
with severe respiratory illness. Strict respiratory isolation was
instituted. Ten days after last exposure, none of 64 close contacts had
developed severe disease, with 13 of 64 reporting mild respiratory
symptoms. The novel coronavirus was not detected in 10 of 10 symptomatic
contacts tested.
The outbreak of severe acute
respiratory syndrome (SARS) in 2003, which led to 8422 cases and 916
deaths worldwide [1], highlighted the potential for newly emerging
zoonotic coronaviruses to transmit from person to person, especially in
healthcare settings, and to cause severe human illness.
On
[22 Sep 2012], the Health Protection Agency (HPA) in London, United
Kingdom (UK), confirmed infection with a novel coronavirus in a patient
in a London hospital who had been transferred from Qatar 11 days
previously. This patient represents the 2nd confirmed case of severe
acute respiratory illness caused by this novel coronavirus. The 1st case
was identified in a Saudi Arabian national who died in June 2012 [2,3].
We describe the exposure history, the public health response and
follow-up of close contacts of the case in London.
Case exposure history and laboratory investigations
The
case is a previously well 49-year-old male who travelled to Saudi
Arabia from [31 Jul 2012 to 18 Aug 2012], where he and several of his
travelling companions developed rhinorrhoea and fever (Figure 1). On [18
Aug 2012], he travelled to Qatar, where his respiratory symptoms
resolved 3 days later. While in Qatar, he spent time on a farm, where he
keeps camels and sheep,
although no direct contact with these animals
was reported.
On [3 Sep 2012], he reported a mild
respiratory illness. Six days later, he required hospitalisation due to
development of bilateral pneumonia. His condition worsened, and he
subsequently required intubation and ventilation. On [12 Sep 2012], he
was transferred by air ambulance to an intensive care unit in London,
where acute renal impairment was also detected. Due to further
deterioration, he was transferred to another London hospital on [20 Sep
2012] [3].
Following the report on ProMED-mail on [20 Sep
2012] [2] of the detection of a novel coronavirus (until further
taxonomic denomination, herewith referred to as hCoV-EMC) in a Saudi
Arabian patient who had died from severe respiratory illness and renal
failure, and as no diagnosis had been established despite investigations
for common causes of pneumonia and pathogens endemic to the Middle
East, the patient in London was investigated for novel coronavirus
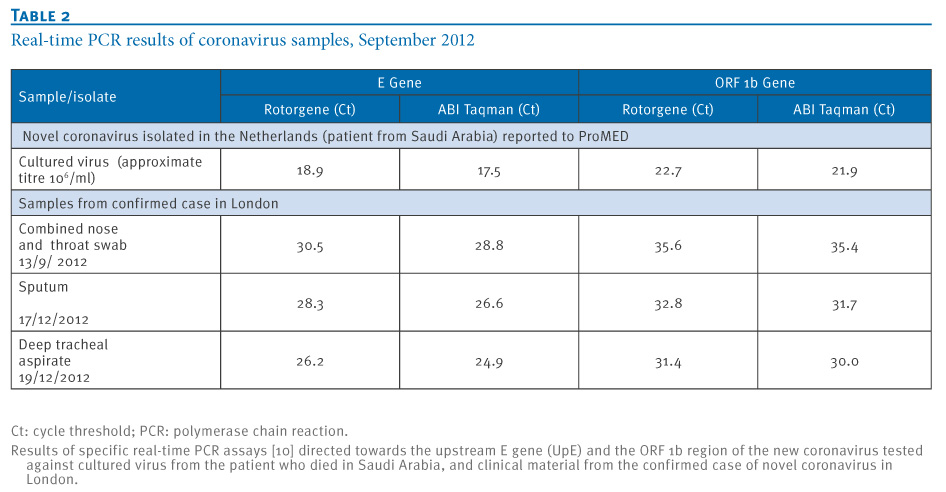
infection. On [21 Sep 2012], a coronavirus was detected in respiratory
tract samples using a pan-coronavirus PCR assay, and on [22 Sep 2012]
sequencing of the PCR amplicon showed a sequence very closely related to
the hCoV-EMC detected in the earlier patient from Saudi Arabia [4]. The
virus belongs to the genus beta-coronavirus, with closest relationship
to bat coronaviruses [4].
Figure 1. Timeline of disease
and travel history of novel coronavirus case, London, August to
September 2012 [available at above URL link]
Public health management
The
identification of a novel coronavirus of the same group as the
SARS-CoV, with 2 clinically severe human cases including one fatality,
led to a public health response being mounted to isolate the case,
identify and test close contacts and to prevent onward transmission.
Once the patient was found to have a novel coronavirus infection, he was
isolated in a negative-pressure single room, and full personal
protective equipment (PPE), including gowns, gloves, eye protection and
high filtration masks were worn by staff and other contacts. Interim
case and close contact definitions were developed [5].
A
possible case was defined as: any person with acute respiratory syndrome
which includes fever (greater than or equal to 38 C), or history of
fever and cough requiring hospitalisation, or with suspicion of lower
airway involvement (clinical or radiological evidence of consolidation)
not explained by another infection or aetiology with history of either
travel to or residence in Saudi Arabia or Qatar, or close contact with a
confirmed case in the 10 days before onset of illness.
A close contact was defined as the following:
-
Healthcare and social care workers: workers who provided direct
clinical or personal care or examination of a symptomatic confirmed case
or within close vicinity of an aerosol generating procedure AND who was
not wearing full personal protective equipment (PPE) at the time. Full
PPE is defined as a correctly fitted high filtration mask (FFP3), gown,
gloves and eye protection.
- Household: any person who had
prolonged face-to-face contact with the confirmed case(s) any time
during the illness after onset in a household setting.
- Other
close contacts: any person who had prolonged face-to-face contact with a
confirmed case while symptomatic in any other enclosed setting and who
was not wearing a mask, e.g. school, visitor to the hospital to the bed
side of a symptomatic confirmed case.
These definitions
were used as the basis for identifying further possible cases and
contacts. Guidelines were developed on the investigation and public
health management of these cases and their close contacts.
Identification
and follow-up of individuals who had close contact with the case at any
time during his symptomatic period from entry into the UK up until
implementation of full isolation on [21 Sep 2012] (including healthcare
workers and family), was rapidly initiated by HPA staff and staff from
the London hospitals' Infection Control Teams. Close contacts were
followed up for a period of 10 days from the date of last exposure to
the index case. If contacts developed respiratory illness in this
period, they were asked to self-isolate in their homes (or were isolated
in hospital if requiring admission).
The hospital in
Qatar was informed to allow them to initiate appropriate follow-up for
those who had been in contact with the patient.
HPA
rapidly developed and published advice to health professionals, the
public and travellers [5]. The case was immediately reported under the
International Health Regulations to the World Health Organisation and
through the European Union Early Warning and Response System (EWRS).
Extensive laboratory work was undertaken to characterise the virus and
develop new diagnostic tools [3].
Initial epidemiological investigation and preliminary findings
Close
contacts of the case were followed up to determine the transmissibility
of this novel coronavirus. This included collection of information on
clinical illness, virological swabbing of contacts who had respiratory
symptoms, and collection of paired sera from all contacts to determine
whether there was evidence of recent infection.
It is
likely that the patient's infection was acquired in Qatar as he was in
Qatar for the 16 days prior to the onset of his most recent respiratory
illness in September [2012]. The earlier, mild upper respiratory tract
infection, which began during his visit to Saudi Arabia, resolved 2
weeks before onset of the present illness.
By [4 Oct
2012], tracing of contacts had identified 64 persons, among healthcare
workers, family and friends, who were reported to have been in close
contact with the confirmed case while he was symptomatic in the UK
(Figure 2).
Ten days after the date of last respective exposure, none of
the close contacts had developed severe respiratory disease requiring
hospital admission. Interim results have identified 13 close healthcare
worker contacts with mild, self-limiting respiratory symptoms. These
contacts were self-isolated in their homes until asymptomatic. In
addition, one hospitalised patient who had potential contact with the
case and subsequently became unwell was identified and subsequently
tested negative using a pan-coronavirus assay [4]. The novel coronavirus
has not been detected in any of the 10 symptomatic healthcare worker
contacts tested by [4 Oct 2012].
Four possible cases with
a history of recent travel from Saudi Arabia or Qatar have also been
identified and investigated in the UK since active case finding
commenced. Although the likelihood of novel coronavirus infection in any
of these was considered low, strict infection control measures were
taken.
For 3 of them, samples were available, and the novel coronavirus
was not detected. A 4th case, who died at the beginning of September
[2012], remains under investigation.
Figure 2. Outcome of
close contact follow-up 10 days or more since last exposure to index
case with a novel coronavirus infection, London, September 2012 (n=64)
[available at above URL link]
Public health implications
We
present a case of severe respiratory illness resulting from a novel
coronavirus acquired in the Middle East. The clinical picture is similar
to that of a case previously described from Saudi Arabia and caused by a
closely related virus. Although cases of SARS, for which the causative
agent SARS-CoV is in the same group of coronaviruses, were reported with
incubation periods beyond 10 days, 95 percent were reported to have an
incubation period of less than 10 days [6]. In the light of this
finding, the case of novel coronavirus that we report appears to have
been acquired in Qatar based on the known time course of the patient's
infection and other available information, unless the illness had an
unusual biphasic nature or a very long incubation period.
After
10 days of follow-up, there has been no confirmed evidence of ongoing
person-to-person transmission resulting in severe disease or milder
laboratory confirmed infection among close contacts, despite extensive
active contact tracing. Completion of case-contact investigation,
including serological testing when available, will determine whether
mild or asymptomatic infection among close contacts has occurred. In
addition, serological investigation in the countries of origin of the 2
confirmed cases should be considered to look for evidence of possible
previous infection in the general population. Studies in animals are
also necessary to determine whether there is an animal reservoir for
this infection and what it might be.
Early detection and
investigation of cases of severe respiratory illness among travellers
returning from countries where infection with novel coronavirus has been
reported and their close contacts will support the further elucidation
of the epidemiological characteristics of this novel virus. An outbreak
of severe respiratory illness of unknown aetiology was reported from the
Middle East earlier in 2012 [7].
Work needs to be undertaken to
determine whether a novel coronavirus has been circulating more widely
in the general population in the Middle East already for some time or
whether the virus was more recently introduced from an unknown animal
reservoir.
References:
1. World Health
Organization (WHO). WHO final summary SARS, 15 August 2003: Summary
table of SARS cases by country, 1 November 2002 - 7 August 2003. Geneva;
WHO; 2003. Available from:
http://www.who.int/csr/sars/country/2003_08_15/en/index.html
2.
ProMED-mail. Novel coronavirus - Saudi Arabia: human isolate. Archive
Number: 20120920.1302733. 20 September 2012. Available from:
http://www.promedmail.org/?p=2400:1000
3.
Corman VM, Eckerle I, Bleicker T, Zaki A, Landt O, Eschbach-Bludau M,
et al. Detection of a novel human coronavirus by real-time
reverse-transcription polymerase chain reaction. Euro Surveill.
2012;17(39):pii=20285. Available from:
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20285
4.
Bermingham A, Chand MA, Brown CS, Aarons E, Tong C, Langrish C, et al.
Severe respiratory illness caused by a novel coronavirus, in a patient
transferred to the United Kingdom from the Middle East, September 2012.
Euro Surveill. 2012;17(40):pii=20290. Available from:
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20290
5.
Health protection Agency (HPA). Algorithm for investigation and
management of possible cases of severe acute respiratory illness
associated with a novel coronavirus. London; HPA; 2012. Available from:
http://www.hpa.org.uk/webw/HPAweb&Page&HPAwebAutoListName/Page/1317136202637
6.
Lessler J, Reich NG, Brookmeyer R, Perl TM, Nelson KE, Cummings DA.
Incubation periods of acute respiratory viral infections: a systematic
review. Lancet Infect Dis. 2009; 9(5):291-300. [abstract available at:
http://www.ncbi.nlm.nih.gov/pubmed/19393959]
7.
European Centres for Disease Control (ECDC). Communicable Disease
Threats Report (Week 18, 29 April-5 May 2012). Stockholm; ECDC: 2012
Available from:
http://ecdc.europa.eu/en/publications/Publications/CDTR%20online%20version%204%20May%202012.pdf
[Reported
by: R G Pebody1, M A Chand1, H L Thomas1,2,3, H K Green1, N L
Boddington1, C Carvalho1,3, C S Brown1, S R Anderson1, C Rooney1, E
Crawley-Boevey1, D J Irwin1, E Aarons4, C Tong4, W Newsholme4, N Price4,
C Langrish4, D Tucker4, H Zhao1, N Phin1, J Crofts1, A Bermingham1, E
Gilgunn-Jones1, K E Brown1, B Evans1, M Catchpole1, J M Watson1
1. Health Protection Agency (HPA), London, United Kingdom
2. Field Epidemiology Training Programme (FETP), Health Protection Agency, London, United Kingdom
3.
European Programme for Intervention Epidemiology Training (EPIET),
European Centre for Disease Prevention and Control, (ECDC), Stockholm,
Sweden
4. Guy's and St Thomas' NHS Foundation Trust and King's Health Partners, London, United Kingdom]






 [PDF - 207 KB]
[PDF - 207 KB]


