Oseltamivir
Evidence suggests that some antiviral drugs, notably oseltamivir, can reduce the duration of viral replication and improve prospects of survival.
In suspected cases, oseltamivir should be prescribed as soon as possible (ideally, within 48 hours following symptom onset) to maximize its therapeutic benefits.[http://www.who.int/mediacentre/factsheets/avian_influenza/en/]
Ceftriaxone injection is used to treat certain infections caused by bacteria such as gonorrhea (a sexually transmitted disease), pelvic inflammatory disease (infection of the female reproductive organs that may cause infertility), meningitis (infection of the membranes that surround the brain and spinal cord), and infections of the lungs, ears, skin, urinary tract, blood, bones, joints, and abdomen. Ceftriaxone injection is also sometimes given before certain types of surgery to prevent infections that may develop after the operation. Ceftriaxone injection is in a class of medications called cephalosporin antibiotics. It works by killing bacteria. Antibiotics will not work for colds, flu, or other viral infections.
Azithromycin is used to treat certain infections caused by bacteria, such as bronchitis; pneumonia; sexually transmitted diseases (STD); and infections of the ears, lungs, skin, and throat. Azithromycin is in a class of medications called macrolide antibiotics. It works by stopping the growth of bacteria. Antibiotics will not work for colds, flu, or other viral infections. (editing is mine).
Excerpt:
Case history
On 14 September 2012, the United Kingdom Health Protection Agency (HPA) Imported Fever Service was notified of a case of unexplained severe respiratory illness in a London intensive care unit. The patient had recently transferred from Qatar and had a history of travel to Saudi Arabia.
He was a previously well 49 year-old man who developed a mild undiagnosed respiratory illness while visiting Saudi Arabia during August 2012, which fully resolved. He subsequently presented to a physician in Qatar on 3 September, with cough, myalgia and arthralgia, and was prescribed oral antibiotics. Five days later, he was admitted to a Qatari hospital with fever (38.4 °C) and hypoxia, with oxygen saturation of 91% on room air. A chest X-ray showed bilateral lower zone consolidation. He was treated with ceftriaxone, azithromycin and oseltamivir. After 48 hours, he required intubation and ventilation and was transferred by air ambulance to London. During transfer, he was clinically unstable, requiring manual ventilation.
On admission to intensive care in London, he remained severely hypoxic, achieving an arterial PaO2 of 6.5 kPA (normal range: 11–13 kPA) on 100% oxygen with optimised pressure ventilation, and required low-dose norepinephrine to maintain blood pressure. His white blood cell count was 9.1 x 109/L (normal range: 4–11 x 109/L), C-reactive protein 350 mg/L (normal range: 0–10 mg/L) and creatinine 353 μmol/L (normal range: 53–97 μmol/L), with normal liver function and coagulation. He was treated with corticosteroids and broad-spectrum antibiotics, initially meropenem, clarithromycin and teicoplanin. Colistin and liposomal amphotericin B were subsequently added.
His condition deteriorated between 11 and 20 September, with progressive hypoxia....
-snip-

Detection of a novel coronavirus
We used real-time PCR on upper (nose and throat swabs) and lower respiratory tract samples (sputum and tracheal aspirates) to test for a range of coronaviruses: OC43, 229E, NL63 and SARS-CoV. We also used a block-based pan-coronavirus PCR with degenerate primers targeted to the conserved RNA-dependent RNA polymerase (RdRp Pol) gene that detects all coronaviruses known to infect humans and a range of animal coronaviruses [6].
The pan-coronavirus assay yielded a band of the correct size in lower respiratory tract samples, but the assays for OC43, 229E, NL63 and SARS-coronaviruses were negative. Sanger sequencing of the pan-coronavirus PCR product (a 251 base pair fragment encompassing nucleotides 104–354 of the NSP12 gene) yielded a sequence that on BLAST analysis gave genetic identity of 81% to bat coronavirus/133/2005 (GenBank accession number DQ648794.1) and 75% identity to porcine haemagglutinating encephalomyelitis virus strain VW572 (GenBank accession number DQ011855.1)
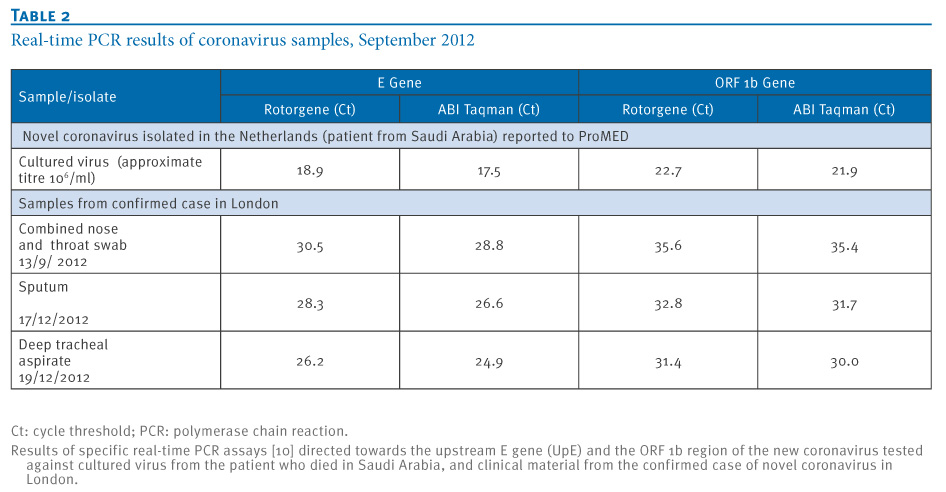
The sequence identified is available on the HPA website [7]. In response to this identification, a new set of real-time RT PCR assays were developed [8]. The results of these assays tested on novel coronavirus tissue culture material and clinical samples from this confirmed case are shown in Table 2.
Table 2. Real-time PCR results of coronavirus samples, September 2012
Click on Table below:
On the basis of the sequence obtained, a maximum likelihood tree (Figure) showed that the virus belongs to the genus Betacoronavirus, with closest relationships to bat coronaviruses HKU4 and HKU5. Viruses that share more than 90% sequence identity in the conserved replicase domain are considered to belong to the same species by the International Committee on Taxonomy of Viruses (ICTV). Our sequence comparisons suggested that the virus nucleic acid fragment identified is derived from a novel coronavirus that is distinct from all coronaviruses described to date.
-snip-
The origin for this novel virus is unknown. Epidemiological human and animal investigations in the region of origin are required to distinguish between an animal reservoir that either directly or indirectly transmits the virus occasionally to humans, and a previously unrecognised endemic infection of humans that causes severe outcomes in a few of those infected. Distinguishing between these possibilities will require wider application of more specific and sensitive molecular assays for coronaviruses, and greater awareness of the possible presence of coronaviruses in human acute severe respiratory illness. Extensive serological testing of potentially exposed human populations and contacts will be a key indicator of the extent of disease due to novel coronaviruses.
Complete document: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20290
No comments:
Post a Comment